 |  |
STATISTICAL BRIEF #319
|
|
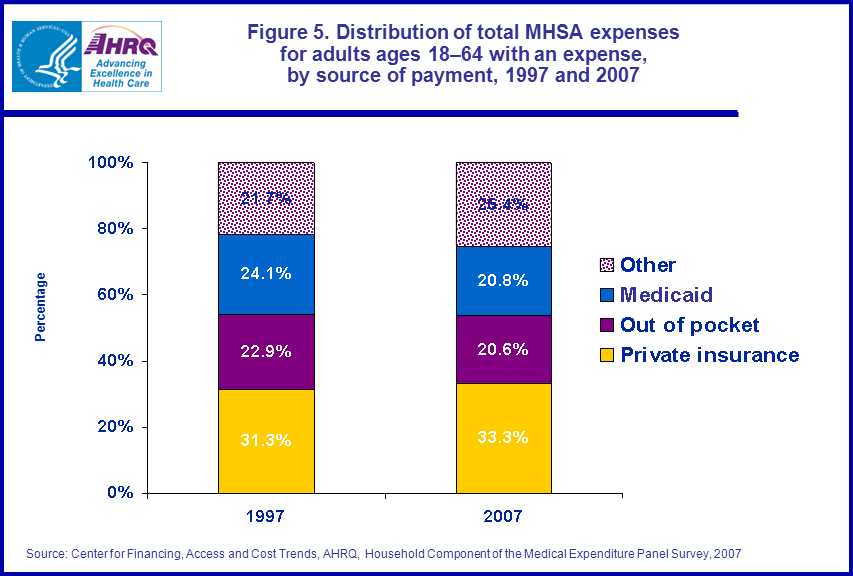
The distribution of total MHSA expenses by source of payment for adults ages 18–64 did not change significantly between 1997 and 2007 (figure 5). In both years, approximately one-third of all medical expenses for adults under age 65 were paid by private insurance.
Data Source
The estimates in this Statistical Brief are based upon data from the 2007 Event-Level Conditions (HC-112), 1997 Event-Level Conditions (HC-018), 2007 Full Year Consolidated (HC-113), and the 1997 Full Year Consolidated (HC-020), public use files.Definitions
Mental Health or Substance Abuse (MHSA) ConditionThis Brief analyzes adults ages 18–64 with a MHSA condition as reported in connection with health care utilization. The conditions reported by respondents were recorded by interviewers as verbatim text, which was then coded by professional coders to fully specified ICD-9-CM codes. These codes were regrouped in clinically homogenous categories known as CCS codes. Conditions with CCS codes 650–659, 662 and 670 (mental health conditions), or 660 and 661 (substance abuse) were used for this Brief. A crosswalk of ICD-9 codes and CCS codes is available in the documentation file of the Medical Conditions File for 2007 (HC-112). For additional information on crosswalk between ICD-9 codes and CCS codes, please visit: http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp.
Expenditures (expenses)
Expenditures include the total direct payments from all sources to hospitals, physicians, other health care providers, and pharmacies for services reported by respondents in the MEPS-HC. Expenditures for hospital-based services include those for both facility and separately billed physician services. Estimates for 1997 were adjusted to 2007 dollars based on the GDP Price Index (http://www.meps.ahrq.gov/mepsweb/about_meps/Price_Index.shtml). Health insurance premiums are not included as expenses.
Type of service
- Office-based: Includes expenses for visits to both physician and non-physician medical providers seen in office settings.
- Hospital inpatient: Includes room and board and all hospital diagnostic and laboratory expenses associated with the basic facility charge, payments for separately billed physician inpatient services, and some emergency room expenses incurred immediately prior to inpatient stays.
- Hospital outpatient: Includes expenses for visits to both physicians and other medical providers seen in hospital outpatient departments, including payments for services covered under the basic facility charge and those for separately billed physician services.
- Emergency room: Includes payments for services covered under the basic facility charge and those for separately billed physician services, but excludes expenses for emergency room services that are included in a hospital inpatient admission.
- Prescribed medicines: Includes expenses for all prescribed medications that were initially purchased or refilled during the year, as well as expenses for diabetic supplies.
- Ambulatory: Combines office-based, hospital outpatient, and emergency room expense categories described above.
- Other: Includes expenses for care in all categories not specified as a separate category, including those for home care and for miscellaneous medical equipment and supplies.
- Out of pocket: This category includes expenses paid by the user or other family member.
- Private insurance: This category includes payments made by insurance plans covering hospital and medical care (excluding payments from Medicare, Medicaid, and other public sources), Medigap plans, or TRICARE (Armed Forces-related coverage). Payments from plans that provide coverage for a single service only, such as dental or vision coverage, are not included.
- Medicaid/SCHIP: Medicaid and SCHIP are means-tested government programs jointly financed by Federal and state funds that provide health care to those who are eligible. Medicaid is designed to provide health coverage to families and individuals who are unable to afford necessary medical care while SCHIP provides coverage to additional low income children not eligible for Medicaid. Eligibility criteria for both programs vary significantly by state.
- Other sources: This category includes payments from Medicare, other miscellaneous Federal sources (Indian Health Service, military treatment facilities, and other care provided by the Federal government); various state and local sources (community and neighborhood clinics, state and local health departments, and state programs other than Medicaid/SCHIP); various unclassified sources (e.g., automobile, homeowners, or other liability insurance, and other miscellaneous or unknown sources); Medicaid/SCHIP payments reported for persons who were not reported as enrolled in the Medicaid or SCHIP programs at any time during the year; and private insurance payments reported for persons without any reported private health insurance coverage during the year.
About MEPS-HC and MEPS-MPC
The MEPS Household Component (HC) is a nationally representative longitudinal survey that collects detailed information on health care utilization and expenditures, health insurance, and health status, as well as a wide variety of social, demographic, and economic characteristics for the U.S. civilian noninstitutionalized population. It is cosponsored by the Agency for Healthcare Research and Quality and the National Center for Health Statistics.The MEPS Medical Provider Component (MPC) collects information on dates of visit, diagnoses and procedures, and charges and payments from a sample of medical providers who provided care to persons in the survey. The MPC data collected are used generally as the primary source of MEPS expenditure data and are also used to impute expenditure information not reported by household respondents.
For more information about MEPS, call the MEPS information coordinator at AHRQ (301) 427-1406 or visit the MEPS Web site at http://www.meps.ahrq.gov/mepsweb.
References
Cohen, J., Cohen S., and Banthin, J. The Medical Expenditure Panel Survey: A National Information Resource to Support Healthcare Cost Research and Inform Policy and Practice. Medical Care 2009, 47(7), Supplement, pp. S44–S50.Cohen, J. Design and Methods of the Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 1. AHCPR Pub. No. 97-0026. Rockville, MD: Agency for Health Care Policy and Research, 1997. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr1/mr1.pdf
Ezzati-Rice, T. M., Rohde, F., Greenblatt, J. Sample Design of the Medical Expenditure Panel Survey Household Component, 1998–2007. Methodology Report No. 22. March 2008. Agency for Healthcare Research and Quality, Rockville, MD. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr22/mr22.pdf
Zuvekas, S. H. Trends in Mental Health Services Use and Spending, 1987–1996. Health Affairs 20(2001): 214–24.HCUP CCS. Healthcare Cost and Utilization Project (HCUP). June 2009. U.S. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp
Suggested Citation
Brown, E. Health Care Expenditures for Adults Ages 18–64 with a Mental Health or Substance Abuse Related Expense: 2007 versus 1997. Statistical Brief #319. March 2011. Agency for Healthcare Research and Quality, Rockville, MD. http://www.meps.ahrq.gov/mepsweb/data_files/publications/st319/stat319.pdfAHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of health care in the United States. We also invite you to tell us how you are using this Statistical Brief and other MEPS data and tools and to share suggestions on how MEPS products might be enhanced to further meet your needs. Please e-mail us at mepspd@ahrq.gov or send a letter to the address below:
Steven B. Cohen, PhD, Director
Center for Financing, Access, and Cost Trends
Agency for Healthcare Research and Quality
540 Gaither Road
Rockville, MD 20850
 |
|
|
 |
|
|
 |
|
|
 |
|
|
 |
|
|