
|
|
|
Font Size:
|
||||
|
|
|
|
||||
STATISTICAL BRIEF #308:
Main Reason for Not Having a Usual Source of Care:
Differences by Race/Ethnicity, Income, and Insurance Status, 2007
Highlights
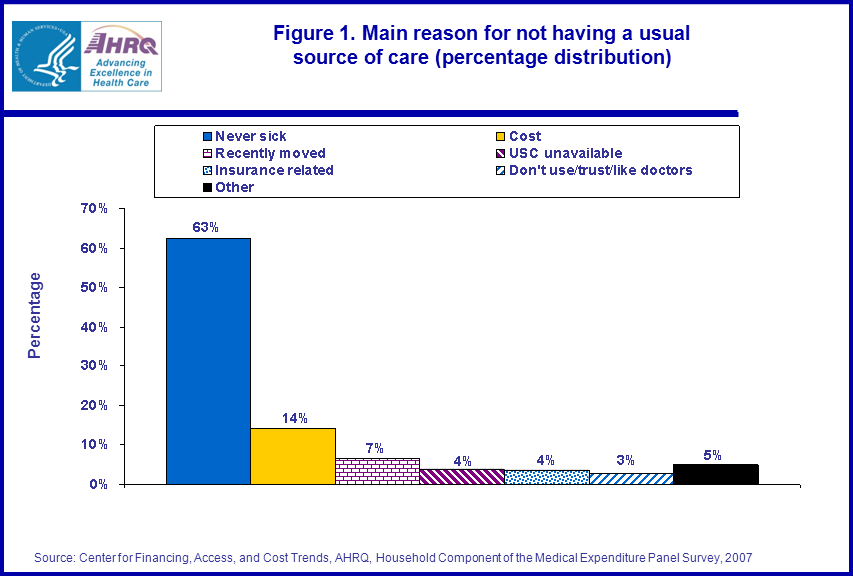
- Across all groups, the most common reason given for not having a USC is, "Seldom or never get sick"; 63 percent of individuals without a usual source of care gave this as their main explanation (figure 1).
- The cost of medical care is the second most common reason given for not having a usual source of care (14 percent).
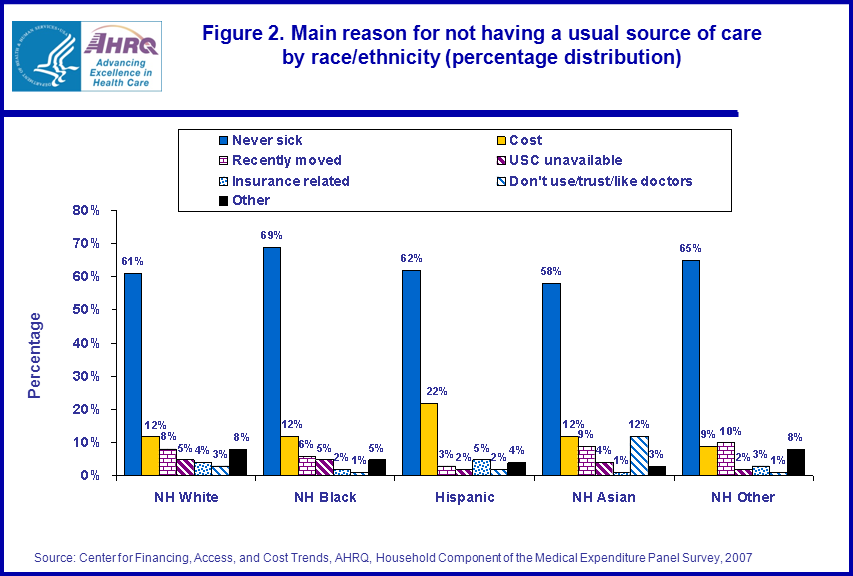
- Hispanics were more likely to report cost as the main reason for not having a usual source of care (22 percent) compared to non-Hispanic (NH) whites (12 percent), NH Asians (12 percent), and NH blacks (12 percent).
- NH Asians were more likely to report that they do not use, trust, or like doctors as the main reason for not having a USC compared to other racial/ethnic groups (12 percent for non-Hispanic Asians versus 3 percent or under for all other racial/ethnic groups).
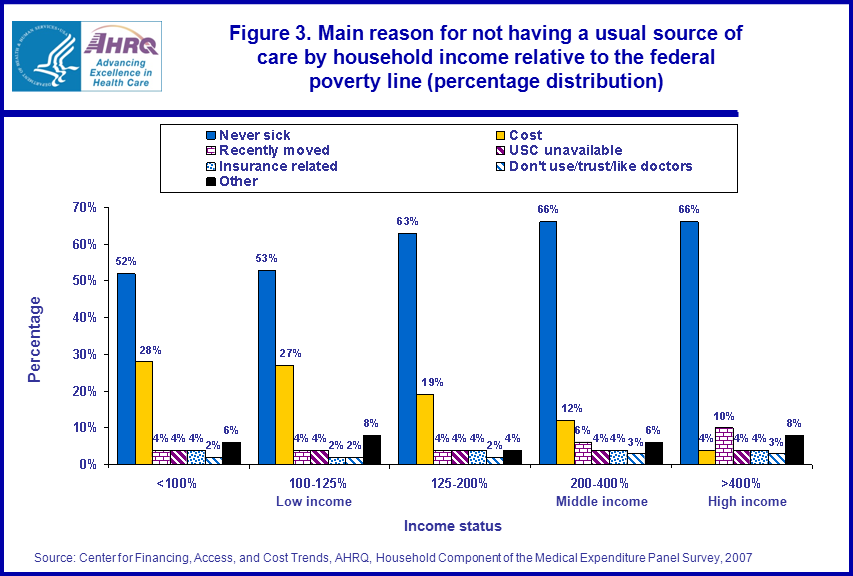
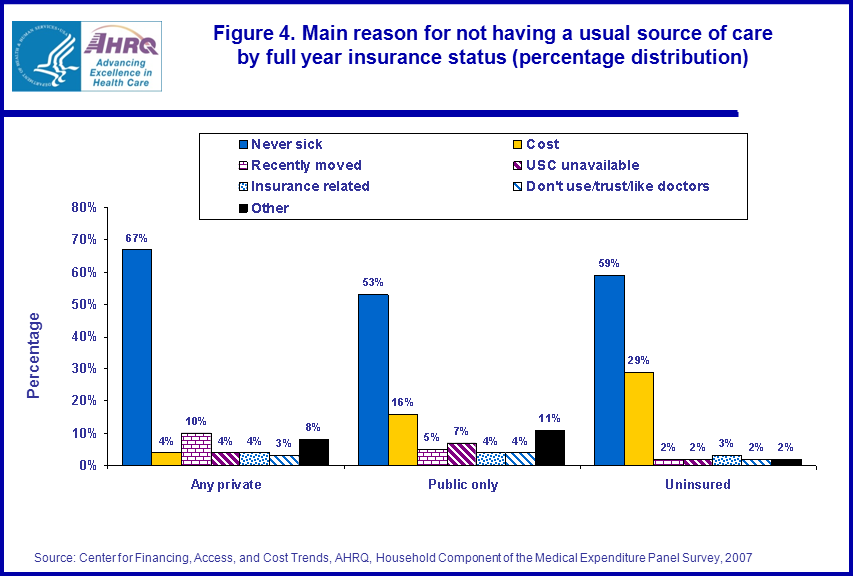
- Individuals without insurance and with low incomes were more likely than others to report cost as the main reason for not having a USC (figures 3 and 4). Even among these individuals, however, "Seldom or never get sick" was still the most common explanation given.
Introduction
Achieving adequate access to ambulatory medical care for all Americans is central to most health care reform proposals. A widely used indicator for access is having a usual source of health care (USC). Differences in the percentage of individuals who do not have a USC by a variety of characteristics including race, ethnicity, income, and insurance status are well documented. Less is known, however, about why individuals do not have a USC and how this differs across the same characteristics. This Statistical Brief explores the main reason given by individuals for not having a USC in 2007 by race, ethnicity, income relative to the federal poverty line, and full-year insurance coverage.Findings
In 2007, among the 20.5 percent of individuals who reported not having a usual source of care, most (63 percent) reported never or seldom getting sick as their main explanation (figure 1). The second most common reason given was the high cost of medical care and about 14 percent of those without a usual source of care reported this as the main explanation. Other reasons given were that individuals had recently moved, couldn't find a doctor, experienced some insurance-related barrier, or that they did not use, like, or trust doctors.Figure 2 indicates that Hispanic individuals without a USC were more likely to report affordability as their main explanation (22 percent) compared to other racial/ethnic groups (12 percent for all other groups). NH Asians were far more likely to report not using, trusting, or liking doctors as their main reason for not having a usual source of care (12 percent) compared to NH whites (3 percent), NH blacks (1 percent), or Hispanics (2 percent).
Differences in the main reason for not having a USC emerged by insurance status and income, too (figure 3 and 4). Not surprisingly, the cost of medical care was more often given as the main reason for not having a USC by those in lower income categories and those with no insurance or public insurance (compared to those with private insurance), and never or seldom getting sick was less often given as the main reason. Nevertheless, even in the poorest income group and among the uninsured and publicly insured, seldom or never getting sick was still the most common explanation offered for not having a usual source of care.
Data Source and Methodology
Estimates for this Brief come from the MEPS HC-113: 2007 Full Year Consolidated Data File. The sample is restricted to those who report having no usual source of care. The main variable was YNOUSC42, and the groups across which statistics were calculated were defined using the variables RACEX, HISPANX, POVCAT, and INSCOV. Standard errors for all estimates are adjusted for complex survey design using the SVY commands in Stata 11.Definitions
Usual source of careIndividuals reported whether or not they or their family member had a particular doctor's office, clinic, health center, or other place (excluding hospital emergency rooms) to go to for medical care when ill or for health-related advice. Individuals who indicated they had a particular place were considered to have a usual source of care.
Main reason for not having a usual source of care
Individuals were asked to report the main reason they did not have a usual source of care. Respondents could select one of several responses, or fill in a response. They could also fill in answers in a subsequent question on the survey regarding "other" reasons for not having a USC. From all these responses, values were assigned to the variable "YNOUSC42." For this Statistical Brief, original values from YNOUS42 were assigned as follows: 1 = "Seldom or never sick", 2 = "Recently moved", 9 = "Cost", 3 and 4 = "USC unavailable", 7 and 10 = "Insurance related", 8, 14 and 20 = "Don't use/trust/like doctors". All other codes were categorized under "other." For more details on YNOUS42, see MEPS documentation and items AC07, AC07OV, and AC08 on the MEPS questionnaire.
Race/ethnicity
Race/ethnicity is coded hierarchically into the following codes: Hispanic regardless of race, non-Hispanic white (no other races reported), non-Hispanic black (no other races reported), non-Hispanic Asian (no other races reported), and non-Hispanic other race or multiple race individuals.
Poverty status
Five income groups are defined based on the percentage of the poverty line for total family income, adjusted for family size and composition: 100 percent, 100-125 percent, 125-200 percent, 200-400 percent, 400 percent. Income is a household-level variable where all sources of income across all earners in the household are summed to form a total income value. This total income value is then divided by the appropriate poverty line income value adjusted for family size and composition.
Low income: persons in families with income less than 200 percent of the federal poverty line (FPL) including persons with negative income. This includes persons classified as poor (less than 100 percent FPL) and near poor (100 percent to less than 125 percent FPL), as well as low income (125 percent FPL to less than 200 percent FPL).
Middle income: persons in families with income over 200 percent through 400 percent of the federal poverty line.
High income: persons in families with income over 400 percent of the federal poverty line.
Insurance status
Insurance status over the entire year is summarized with three mutually exclusive categories: any private insurance, public only, and uninsured. The private insurance category is made up of individuals who had any private insurance coverage during the year. The public category is composed of individuals who never had private insurance but were covered by public insurance for at least part of the year. Finally, individuals in the uninsured category had no insurance for the entire year.
About MEPS-HC
MEPS-HC is a nationally representative longitudinal survey that collects detailed information on health care utilization and expenditures, health insurance, and health status, as well as a wide variety of social, demographic, and economic characteristics for the U.S. civilian noninstitutionalized population. It is cosponsored by the Agency for Healthcare Research and Quality and the National Center for Health Statistics.References
For a detailed description of the MEPS-HC survey design, sample design, and methods used to minimize sources of nonsampling error, see the following publications:Cohen, J. Design and Methods of the Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 1. AHCPR Pub. No. 97-0026. Rockville, MD: Agency for Health Care Policy and Research, 1997. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr1/mr1.shtml
Cohen, S. Sample Design of the 1996 Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 2. AHCPR Pub. No. 97-0027. Rockville, MD: Agency for Health Care Policy and Research, 1997. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr2/mr2.shtml
Cohen, S. Design Strategies and Innovations in the Medical Expenditure Panel Survey. Medical Care, July 2003: 41(7) Supplement: III-5-III-12.
Suggested Citation
Kirby, James B. Main Reason for Not Having a Usual Source of Care by Race, Ethnicity, Income, and Insurance Status, 2007. December 2010. Agency for Healthcare Research and Quality, Rockville, MD. http://meps.ahrq.gov/mepsweb/data_files/publications/st308/stat308.shtmlAHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of health care in the United States. We also invite you to tell us how you are using this Statistical Brief and other MEPS data and tools and to share suggestions on how MEPS products might be enhanced to further meet your needs. Please e-mail us at mepspd@ahrq.gov or send a letter to the address below:
Steven B. Cohen, PhD, Director
Center for Financing, Access, and Cost Trends
Agency for Healthcare Research and Quality
540 Gaither Road
Rockville, MD 20850
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||