
|
|
|
Font Size:
|
||||
|
|
|
|
||||
Sources of Health Insurance among Adults with Long COVID: Estimates from the Medical Expenditure Panel Survey
Research Findings #53 | September 2025
Thomas M. Selden, PhD, Zhengyi Fang, MS, and Steven C. Hill, PhD
Highlights
- In early 2024, 3.4 percent of U.S. civilian, noninstitutionalized adults currently had Long COVID, and 2.4 percent had activity-limiting Long COVID.
- Among those diagnosed with chronic respiratory conditions 7.5 percent of adults with pre-pandemic emphysema had Long COVID, and 6.2 percent of adults with pre-pandemic asthma had Long COVID.
- Among adults aged 18 to 64 with Long COVID, 65.3 percent had private insurance or TRICARE, 23.2 percent had public coverage, and 11.3 percent were uninsured.
- Among adults aged 18 to 64 with activity-limiting Long COVID, 62.4 percent had private insurance or TRICARE, 25.7 percent had public coverage, and 11.9 percent were uninsured.
- Among adults aged 65 or older with Long COVID, 42.2 percent had both Medicare and private insurance, 11.6 percent had Medicare and additional public coverage, 42.1 percent had Medicare alone, and 4.1 percent did not have Medicare.
Abstract
This Research Findings uses data from the Medical Expenditure Panel Survey (MEPS-HC) to estimate the prevalence of ongoing symptoms after coronavirus disease 2019 ("Long COVID"), the prevalence of activity-limiting Long COVID, and the prevalence of sources of health insurance among adults reporting Long COVID and activity-limiting Long COVID.
Introduction
In this Research Findings, data from the nationally representative Household Component of the Agency for Healthcare Research and Quality's (AHRQ) Medical Expenditure Panel Survey (MEPS-HC) are used to estimate (1) the prevalence of ongoing symptoms after coronavirus disease 2019 ("Long COVID") among adults, by sociodemographic characteristics and by chronic conditions that they had before 2020 ("pre-pandemic conditions"), (2) the prevalence of activity-limiting Long COVID,1 and (3) the prevalence of sources of health insurance among adults reporting Long COVID and activity-limiting Long COVID. For sources of insurance, this Research Findings differentiates between elderly and nonelderly adults because sources of insurance change when adults turn 65 and become eligible for Medicare. It complements earlier research on the prevalence of Long COVID2 and health insurance among nonelderly adults with Long COVID.3 All differences discussed in the text are statistically significant at the 0.05 level.
Medical Expenditure Panel Survey
MEPS-HC is a nationally representative longitudinal survey that collects detailed information on health care utilization and expenditures, health insurance, and health status, as well as a wide variety of social, demographic, and economic characteristics for the U.S. civilian noninstitutionalized population. It is cosponsored by the Agency for Healthcare Research and Quality and the National Center for Health Statistics.
The MEPS has an overlapping panel design. The data in this Research Findings were collected in the spring of 2024 in the third interview of panel 28 and the fifth interview of panel 27 and were publicly released in the 2023 MEPS-HC Full-Year Consolidated Data File.
The MEPS first started asking questions about Long COVID in the spring of 2023. This Research Findings uses responses from the second time the questions were fielded, in the spring of 2024. The series of questions asks respondents to report household members who have symptoms lasting 3 months or longer that they did not have before a COVID-19 infection. Adults who had these symptoms at the time of the interview are classified as having Long COVID in this Research Findings. Those who reported their symptoms reduced their day-to-day activities are classified as having activity-limiting Long COVID.
Findings
Prevalence of Long COVID (Table 1)
In early 2024, 3.4 percent of U.S. civilian noninstitutionalized adults currently had Long COVID. Table 1 shows the variation in the prevalence of Long COVID across several subgroups.
The prevalence of Long COVID was correlated with pre-pandemic conditions, especially respiratory conditions and heart disease. The prevalence was 7.5 percent among adults with pre-pandemic emphysema, 6.2 percent among adults with pre-pandemic asthma, and 5.9 percent among adults with pre-pandemic heart disease. This Research Findings utilized information about nine pre-pandemic chronic conditions, and among those with two or more of the nine conditions, 5.5 percent had Long COVID, more than twice the prevalence among those with none of the nine pre-pandemic conditions (2.3%).
Long COVID was more prevalent among women (4.2%) than men (2.5%), and it was more prevalent among non-Hispanic White adults (3.9%) than among Hispanic adults (2.6%) or non-Hispanic Black adults (1.9%). Long COVID was more prevalent in rural areas (4.6%) than urban area (3.2%), where urban areas are metropolitan statistical areas (MSAs). Long COVID was more prevalent in the Midwest (3.7%) and West (4.0%) than in the Northeast (2.7%). Differences in prevalence across the four categories of the income distribution studied were not statistically significant.
Prevalence of activity-limiting Long COVID (Table 2)
The impact of Long COVID can vary across individuals. The MEPS-HC asks those reporting Long COVID how much their long-term symptoms reduce their "...ability to carry out day-to-day activities compared with the time before [they] had COVID-19?" In early 2024, 2.4 percent of adults (about 70 percent of adults who reported Long COVID) had any activity-limiting Long COVID.
The prevalence of activity-limiting Long COVID was also correlated with pre-pandemic conditions, especially respiratory conditions and cardiovascular diseases. The prevalence was 7.0 percent among adults with pre-pandemic emphysema, 4.9 percent among adults with pre-pandemic asthma, 4.6 percent among adults with pre-pandemic heart disease, and 5.0 percent among adults who had ever had a stroke before 2020. The prevalence of activity-limiting Long COVID was 4.0 percent among those with two or more of nine conditions before the pandemic, 2.4 percent among those with one pre-pandemic condition, and 1.5 percent among those with none of the nine pre-pandemic conditions.
Activity-limiting Long COVID was more prevalent among women (2.9%) than men (1.8%), and it was more prevalent among non-Hispanic White adults (2.7%) than among those who were Hispanic (1.8%) or non-Hispanic Black (1.0%). Activity-limiting Long COVID was more prevalent in the West (3.0%) than in the Northeast (1.7%). Adults in families with income below 125 percent of the poverty line were more likely than families with incomes 400 percent of the poverty line or higher to have activity-limiting Long COVID (3.4% versus 2.1%).
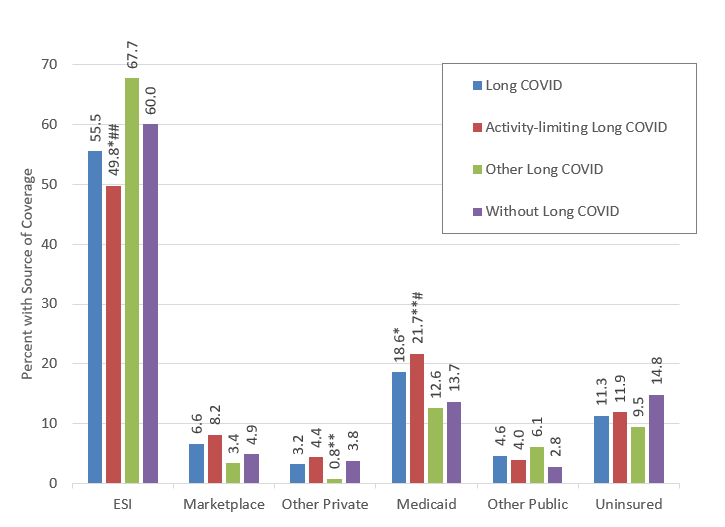
Insurance coverage for the nonelderly (Figure 1)
Among nonelderly adults (aged 18 to 64) with Long COVID, 65.3 percent had private insurance or TRICARE, 23.2 percent had public coverage, and 11.3 percent were uninsured. Examining private insurance and TRICARE in greater detail, 55.5 percent of adults with Long COVID had employer sponsored insurance (ESI) or TRICARE, 6.6 percent had insurance through the Marketplaces, and 3.2 percent purchased individual insurance off the Marketplaces or did not know whether they obtained it. Medicaid accounted for most of the public coverage, 18.6 percent of adults with Long COVID.
Nonelderly adults with Long COVID were significantly more likely to have been enrolled in Medicaid than those without Long COVID. The difference can be explained by lower rates of uninsurance and ESI coverage among those with Long COVID - however, the rates of ESI coverage and the uninsurance rates were not by themselves statistically significantly different between nonelderly adults with and without Long COVID.
Among nonelderly adults with activity-limiting Long COVID, 62.4 percent had private insurance or TRICARE, 25.7 percent had public coverage, and 11.9 percent were uninsured. Those with activity-limiting Long COVID had a lower rate of ESI coverage and a higher rate of Medicaid coverage than those whose Long COVID did not limit their activities.
Insurance coverage for the elderly (Figure 2)
Among elderly adults (age 65 or older) with Long COVID, 42.2 percent had both Medicare and private insurance, 11.6 percent had Medicare and additional public coverage, 42.1 percent had Medicare alone, and 4.1 percent did not have Medicare, although they may have other sources of insurance. None of the differences between elders with and without Long COVID are statistically significant. Note also that small cell sizes precluded the presentation of estimates for elders with activity-limiting Long COVID.
Discussion
Among civilian, noninstitutionalized adults, the population prevalence estimate for Long COVID from the MEPS-HC (3.4%) is the same as the estimate from the National Health Interview Survey for 2022, the source for the questions in the MEPS-HC.2 In addition, estimates from the two surveys were similar in terms of (1) prevalence for demographic subgroups and (2) sources of insurance among the nonelderly.3 The correlation between pre-pandemic conditions and Long COVID is consistent with an earlier study.4
Estimates in this Research Findings are descriptive in nature and have not been adjusted for difference in age, sex, or other socioeconomic characteristics. Also, further study is needed to understand the directions of causality between health insurance coverage and having long COVID.
Definitions
Adults
Aged 18 or older (1) 12/31/2023 (or earlier if the adult left the MEPS before the end of 2023) for panel 27, or (2) at the time of the end of the reference period for the first interview of 2024 for panel 28.
Age groups
Elderly: Aged 65 or older (1) 12/31/2023 (or earlier if the adult left the MEPS before the end of 2023) for panel 27, or (2) at the time of the end of the reference period for the first interview of 2024 for panel 28.
Nonelderly: Aged 18 to 64 (1) 12/31/2023 (or earlier if the adult left the MEPS before the end of 2023) for panel 27, or (2) at the time of the end of the reference period for the first interview of 2024 for panel 28.
Long COVID
Adults are classified as having Long COVID based on answers to a series of questions. For each person in the household, the MEPS asks whether they had ever had COVID-19. If they have ever had COVID-19, the MEPS asks whether they had "symptoms lasting 3 months or longer that [they] did not have prior to having COVID-19?" If the respondent answers affirmatively, the next question is whether they "have symptoms now?" Those with current symptoms as of the interview date are designated as having Long COVID.
Activity-limiting Long COVID
For each adult with Long COVID, the MEPS-HC asks how much the long-term symptoms reduce their "...ability to carry out day-to-day activities compared with the time before [they] had COVID-19? Would you say not at all, a little, a lot, or somewhere in between a little and a lot?" Adults with activity-limiting Long COVID are comprised of those with answers of a little, a lot, or somewhere in between a little and a lot. Adults whose Long COVID did not limit activities are those who said not at all. The response for one nonelderly sample member was "don't know," and that observation was excluded from estimates using this question.
Pre-pandemic chronic conditions
The MEPS asks whether each family member was ever diagnosed with arthritis, asthma, cancer, diabetes, emphysema, high blood pressure, high cholesterol, stroke, a heart attack, angina, coronary heart disease, and other heart disease. For each condition reported, the MEPS asks how old the person was when they were first diagnosed. Using the person's date of birth, conditions first diagnosed before 2020 are classified as pre-existing before the COVID-19 pandemic. A person is classified as having pre-pandemic heart disease if they had a heart attack before 2020 or pre-pandemic angina, coronary heart disease, or other heart disease.
Insurance coverage for the nonelderly
For adults under age 65, insurance coverage categories are (1) 12/31/2023 (or earlier if the adult left the MEPS before the end of 2023) for panel 27, or (2) at the time of the end of the reference period for the first interview of 2024 for panel 28. Categories are assigned hierarchically as follows: ESI or TRICARE (which is Armed Forces-related coverage), Marketplace, any other private insurance (which includes individual insurance obtained outside the Marketplace and private insurance from unknown sources), Medicaid, any other public coverage, and uninsured.
ESI is insurance from a current or former employer (either their own or another person's employer) that provided coverage for hospital and physician care.
The uninsured are defined as people not covered by Medicaid, Medicare, TRICARE, other public hospital/physician programs, private hospital/physician insurance, or insurance purchased through health insurance Marketplaces. People covered only by non-comprehensive state-specific programs (e.g., Maryland Kidney Disease Program) or private, single-service plans, such as coverage for dental or vision care only, or coverage for accidents or specific diseases, were considered uninsured.
Insurance coverage for the elderly
For adults age 65 and over, insurance coverage categories (1) 12/31/2023 (or earlier if the adult left the MEPS before the end of 2023) for panel 27 or (2) at the time of the end of the reference period for the first interview of 2024 for panel 28. Categories are assigned as follows:
- Medicare only: A person is classified as Medicare only if they were covered by Medicare only.
- Medicare and private: A person is classified as having Medicare and private health insurance coverage if they were covered by Medicare and had private insurance that provided coverage for hospital and physician care (including Medigap coverage and TRICARE).
- Medicare and public only: A person is classified as having Medicare and public only insurance if they were covered by Medicare, they were not covered by private insurance or TRICARE, and they were covered by Medicaid or other public hospital and physician coverage.
- No Medicare: A person is classified as having no Medicare if they reported no Medicare coverage.
Race/Ethnicity
Classification by race/ethnicity was based on information reported for each family member. First, respondents were asked if the person's main national origin or ancestry was Puerto Rican; Cuban; Mexican, Mexican American, or Chicano; other Latin American; or other Spanish. All people whose main national origin or ancestry was reported in one of these Hispanic groups, regardless of racial background, were classified as Hispanic. All other people were classified according to their reported race. For this analysis, the following classification by race and ethnicity was used: Hispanic, non-Hispanic Black, non-Hispanic White, and non-Hispanic other. Due to small sample sizes, results are not shown for non-Hispanic adults of other races, which included American Indian, Alaska Native, Asian or Pacific Islander, other race, and multiple races.
Urbanicity
Metropolitan Statistical Area (MSA) is based on the location of the household at the time of their spring 2024 interview and reflects the most recent delineations of MSAs established by the Office of Management and Budget (OMB). An MSA contains a core urban area with a population of 50,000 or more. All counties that are not part of an MSA are considered rural.
Region
Each MEPS household was classified as belonging to one of four regions as defined by the U.S. Census Bureau at the time of their spring 2024 interview:
Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont
Midwest: Indiana, Illinois, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin
South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia
West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming
Poverty Status
Each sample member was classified according to the total annual income of their family in 2023. Possible sources of income included annual earnings from wages, salaries, bonuses, tips, and commissions; business and farm gains and losses; unemployment and Workers' Compensation; interest and dividends; alimony, child support, and other private cash transfers; private pensions, individual retirement account withdrawals, Social Security benefits, and Department of Veterans Affairs payments; Supplemental Security Income and cash welfare payments from public assistance, and Aid to Families with Dependent Children; gains or losses from estates, trusts, partnerships, S corporations, rent, and royalties; and a small amount of "other" income. Poverty status is the ratio of family income to the corresponding federal poverty thresholds, which control for family size and the age of the head of the family. For example, the 2023 poverty threshold for a family of two adults with two children was $30,900. Categories are defined as follows:
- Poor or near poor: Household income below 125 percent of the federal poverty line
- Low income: 125 percent to less than 200 percent of the poverty line
- Middle income: 200 percent to less than 400 percent of the poverty line
- High income: Greater than or equal to 400 percent of the poverty line
Data Source
The estimates shown in this Research Findings are based on data from the MEPS asked in the spring of 2024 and available on the 2023 Full-Year Consolidated Data File (H251). This data file is publicly available from this site: https://meps.ahrq.gov/data_stats/download_data_files.jsp.
References
1 Vahratian A, Saydah, S, Betolli J, Unger ER, Gregory CO. "Prevalence of Post-COVID-19 Condition and Activity-Limiting Post-COVID-19 Condition Among Adults." JAMA Network Open 2024; 7(12):e2451151.
2 Adjaye-Gbewonyo D, Vahratian A, Gregory CO, Betolli J. Long COVID in Adults: United States, 2022. NCHS Data Brief no. 480. Hyattsville, MD: National Center for Health Statistics. 2023. DOI: https://dx.doi.org/10.15620/cdc:132417
3 Ford ND, Slaughter D, Dalton AF, Edwards D, Ma K, King H, Saydah S. "Health Insurance and Access to Care in U.S. Working-Age Adults Experiencing Long COVID." American Journal of Preventive Medicine. 2024 October;67(4):530-539. DOI: 10.1016/j.amepre.2024.05.007
4 Fang Z, Ahrnsbrak R, Rekito A. "Evidence Mounts That About 7% of US Adults Have Had Long COVID." JAMA. 2024;332(1):5-6. doi:10.1001/jama.2024.11370
The following Methodology Reports contain information on the survey and sample designs for the MEPS Household Component (HC).
Cohen, J. Design and Methods of the Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 1. AHCPR Pub. No. 97-0026. Rockville, MD. Agency for Healthcare Policy and Research, 1997. https://meps.ahrq.gov/data_files/publications/mr1/mr1.pdf
Ezzati-Rice, T.M., Rohde, F., Greenblatt, J., Sample Design of the Medical Expenditure Panel Survey Household Component, 1998-2007. Methodology Report No. 22. March 2008. Agency for Healthcare Research and Quality, Rockville, MD. https://meps.ahrq.gov/mepsweb/data_files/publications/mr22/mr22.pdf
Machlin, S.R., Chowdhury, S.R., Ezzati-Rice, T., DiGaetano R., Goksel H., Wun L.M., Yu W., Kashihara D. Estimation Procedures for the Medical Expenditure Panel Survey Household Component. Methodology Report #24. September 2010. Agency for Healthcare Research and Quality, Rockville, MD. https://meps.ahrq.gov/mepsweb/data_files/publications/mr24/mr24.shtml
Suggested Citation
Selden, T.M., Fang, Z., and Hill, S.C. Sources of Health Insurance among Adults with Long COVID: Estimates from the Medical Expenditure Panel Survey. Research Findings #53. September 2025. Agency for Healthcare Research and Quality, Rockville, MD. https://meps.ahrq.gov/data_files/publications/rf53/rf53.pdf
AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Research Finding and other MEPS data and tools and to share suggestions on how MEPS products might be enhanced to further meet your needs. Please email MEPSProjectDirector@ahrq.hhs.govor send a letter to the address below:
Samuel H. Zuvekas, PhD, Acting Director
Center for Financing, Access and Cost Trends
Agency for
Healthcare Research and Quality
5600 Fishers Lane, Mailstop 07W41A
Rockville, MD 20857
Tables and Figures
Table 1. Prevalence of Long COVID, early 2024
| Percent | Standard Error | Notes | |
|---|---|---|---|
| All adults | 3.4 | 0.18 | |
| Adults with pre-pandemic respiratory conditions | |||
| Asthma | 6.2 | 0.59 | ** |
| Emphysema | 7.5 | 2.03 | * |
| Adults with pre-pandemic cardiovascular conditions | |||
| Heart disease | 5.9 | 0.67 | ** |
| High blood pressure | 4.9 | 0.42 | ** |
| High cholesterol | 5.0 | 0.48 | ** |
| Stroke | 5.2 | 1.09 | |
| Adults with other pre-pandemic conditions | |||
| Arthritis | 5.5 | 0.50 | ** |
| Cancer | 4.3 | 0.58 | |
| Diabetes | 5.3 | 0.74 | ** |
| Number of pre-pandemic conditions | |||
| None | 2.3 | 0.21 | Ref |
| One | 3.1 | 0.36 | |
| Two or more | 5.5 | 0.43 | ** |
| Age | |||
| 18 to 64 | 3.4 | 0.20 | Ref |
| 65 or older | 3.5 | 0.35 | |
| Sex | |||
| Male | 2.5 | 0.22 | Ref |
| Female | 4.2 | 0.26 | ** |
| Race and Ethnicitya | |||
| Hispanic | 2.6 | 0.32 | ** |
| Non-Hispanic White | 3.9 | 0.25 | Ref |
| Non-Hispanic Black | 1.9 | 0.34 | ** |
| Non-Hispanic Asian | 2.7 | 0.66 | |
| Urbancity | |||
| MSA | 3.2 | 0.18 | Ref |
| Non-MSA | 4.6 | 0.58 | * |
| Region | |||
| Northeast | 2.7 | 0.33 | Ref |
| Midwest | 3.7 | 0.37 | * |
| South | 3.2 | 0.31 | |
| West | 4.0 | 0.41 | * |
| Poverty status | |||
| Poor/near poor | 4.2 | 0.48 | |
| Low income | 3.5 | 0.55 | |
| Middle income | 3.3 | 0.32 | |
| High income | 3.2 | 0.24 | Ref |
Source: Medical Expenditure Panel Survey Household Component, Early 2024.
Notes: a Results not shown for non-Hispanic adults of other races, including those of multiple races, due to small sample sizes.
* and ** denote significantly different from the reference group (denoted Ref) or, for the pre-pandemic conditions, adults who did not have the pre-pandemic condition at p < .05 and p < .01, respectively.
Table 2. Prevalence of Activity-limiting Long COVID, early 2024
| Percent | Standard Error | Notes | |
|---|---|---|---|
| All adults | 2.4 | 0.15 | |
| Adults with pre-pandemic respiratory conditions | |||
| Asthma | 4.9 | 0.56 | ** |
| Emphysema | 7.0 | 2.17 | * |
| Adults with pre-pandemic cardiovascular conditions | |||
| Heart disease | 4.6 | 0.62 | ** |
| High blood pressure | 3.4 | 0.35 | ** |
| High cholesterol | 3.5 | 0.38 | ** |
| Stroke | 5.0 | 1.07 | * |
| Adults with other pre-pandemic conditions | |||
| Arthritis | 3.9 | 0.45 | ** |
| Cancer | 3.3 | 0.54 | |
| Diabetes | 3.6 | 0.51 | ** |
| Number of pre-pandemic conditions | |||
| None | 1.5 | 0.16 | Ref |
| One | 2.4 | 0.32 | * |
| Two or more | 4.0 | 0.38 | ** |
| Age | |||
| 18 to 64 | 2.3 | 0.17 | Ref |
| 65 or older | 2.8 | 0.32 | |
| Sex | |||
| Male | 1.8 | 0.19 | Ref |
| Female | 2.9 | 0.21 | ** |
| Race and Ethnicitya | |||
| Hispanic | 1.8 | 0.28 | ** |
| Non-Hispanic White | 2.7 | 0.21 | Ref |
| Non-Hispanic Black | 1.0 | 0.22 | ** |
| Non-Hispanic Asian | 2.5 | 0.65 | |
| Urbancity | |||
| MSA | 2.2 | 0.16 | Ref |
| Non-MSA | 3.3 | 0.51 | |
| Region | |||
| Northeast | 1.7 | 0.28 | Ref |
| Midwest | 2.4 | 0.34 | |
| South | 2.3 | 0.28 | |
| West | 3.0 | 0.35 | ** |
| Poverty status | |||
| Poor/near poor | 3.4 | 0.44 | ** |
| Low income | 2.9 | 0.53 | |
| Middle income | 2.2 | 0.25 | |
| High income | 2.1 | 0.20 | Ref |
Source: Medical Expenditure Panel Survey Household Component, Early 2024.
Notes: a Results not shown for non-Hispanic adults of other races, including those of multiple races, due to small sample sizes.
* and ** denote significantly different from the reference group (denoted Ref) or, for the pre-pandemic conditions, adults who did not have the pre-pandemic condition at p < .05 and p < .01, respectively.
Figure 1. Health Insurance Coverage by Presence of Long COVID and Activity-Limiting Long COVID, Adults Aged 18-64 in Early 2024
| Source of Coverage | Long COVID | Activity-limiting Long COVID | Other Long COVID | Without Long COVID |
|---|---|---|---|---|
| ESI (Employer-Sponsored Insurance) | 55.5 | 49.8*## | 67.7 | 60.0 |
| Marketplace | 6.6 | 8.2 | 3.4 | 4.9 |
| Other Private | 3.2 | 4.4 | 0.8** | 3.8 |
| Medicaid | 18.6* | 21.7**# | 12.6 | 13.7 |
| Other Public | 4.6 | 4.0 | 6.1 | 2.8 |
| Uninsured | 11.3 | 11.9 | 9.5 | 14.8 |
Source: Medical Expenditure Panel Survey Household Component, Early 2024.
Notes: ESI = employer sponsored insurance. Other Long COVID = Long COVID that did not limit activities.
* and ** denote significantly different from adults without Long COVID at p < .05 and p < .01, respectively.
# and ## denote significantly different from adults with Long COVID that did not limit activities at p < .05 and p < .01, respectively.
Figure 2. Health Insurance Coverage by Presence of Long COVID, Adults Aged 65+ in Early 2024
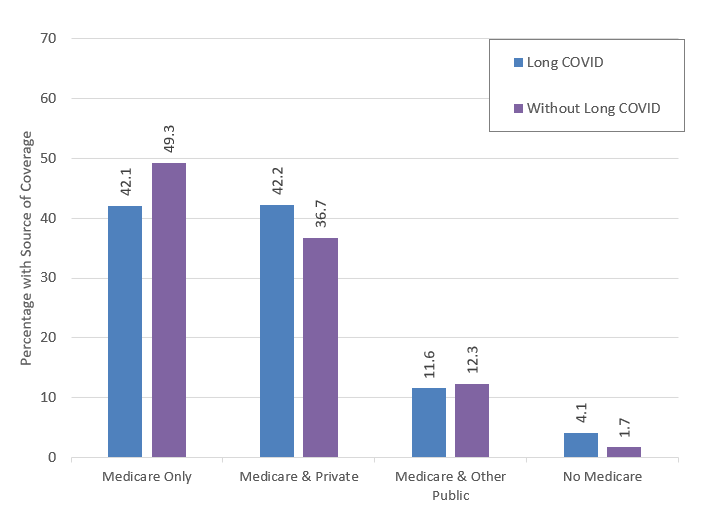
| Source of Coverage | Long COVID | Without Long COVID |
|---|---|---|
| Medicare Only | 42.1 | 49.3 |
| Medicare & Private | 42.2 | 36.7 |
| Medicare & Other Public | 11.6 | 12.3 |
| No Medicare | 4.1 | 1.7 |
Source: Medical Expenditure Panel Survey Household Component, Early 2024.
Note: None of the differences between elderly adults with and without Long COVID are statistically significant.
AHRQ Pub. No. 25-0086
September 2025