Skip to main content

|
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
STATISTICAL BRIEF #529:
|
||||||||||||||||||||||||||||||
| April 2020 | ||||||||||||||||||||||||||||||
| Yao Ding, PhD and G. Edward Miller, PhD
|
||||||||||||||||||||||||||||||
Highlights
|
||||||||||||||||||||||||||||||
IntroductionPrescription opioids are essential to help manage acute or chronic pain in millions of Americans. However, misuse or abuse of these opioid products which can result in drug dependence, overdose, and mortality, has become a national public health crisis in the past few years.1 Examining expenses, utilization and financing of prescribed opioids can help inform the efforts to address the crisis.This Statistical Brief examines opioid utilization and expenditures by adults (ages 18 and older) in the U.S. civilian noninstitutionalized population. We present Medical Expenditure Panel Survey (MEPS) Household Component (HC) estimates of total expenses, total fills and sources of payment for all outpatient prescription opioids, as well as the same measures for the top five opioid products ranked by total expenses in 2017 (hydrocodone, oxycodone, tramadol, morphine, and codeine). We include all opioid medications that are commonly used to treat pain but exclude respiratory agents, antitussives, and medicines commonly used in Medication Assisted Treatment. Only prescriptions purchased or obtained in an outpatient setting (retail and mail-order prescribed medicines) are included in these estimates. Prescription medicines administered in an inpatient setting or in a clinic or physician's office are excluded. All differences between estimates discussed in the text are statistically significant at the 0.05 level. Because of methodological and definitional differences, readers should use caution when comparing MEPS estimates of opioid expenditures and utilization with estimates from other sources. Details on the MEPS methodology and differences with other sources are included in the Definitions section of this Statistical Brief. |
||||||||||||||||||||||||||||||
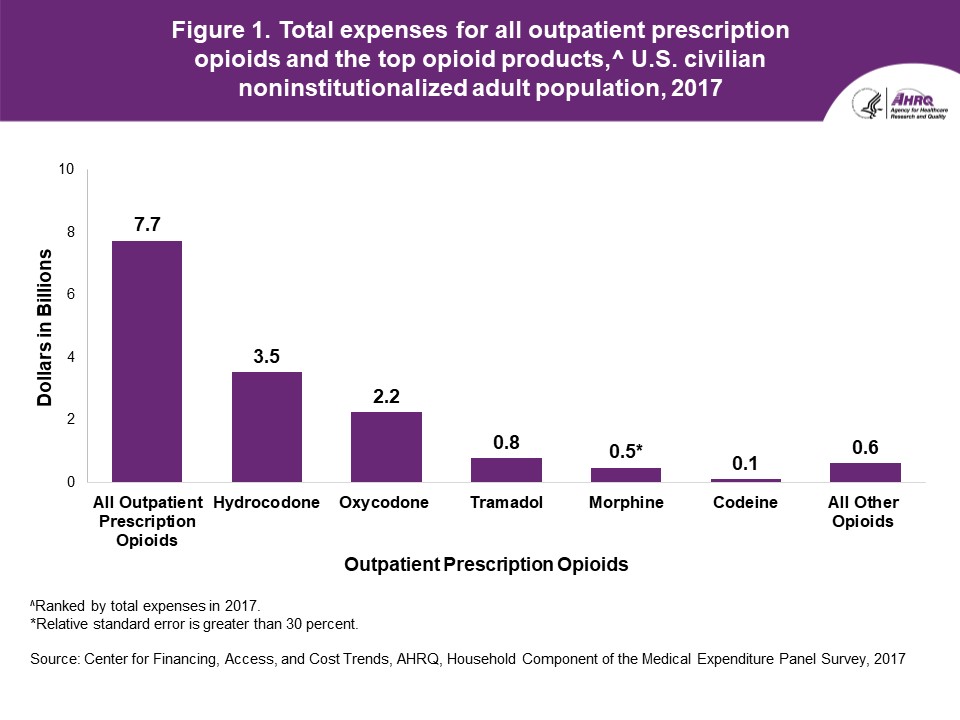
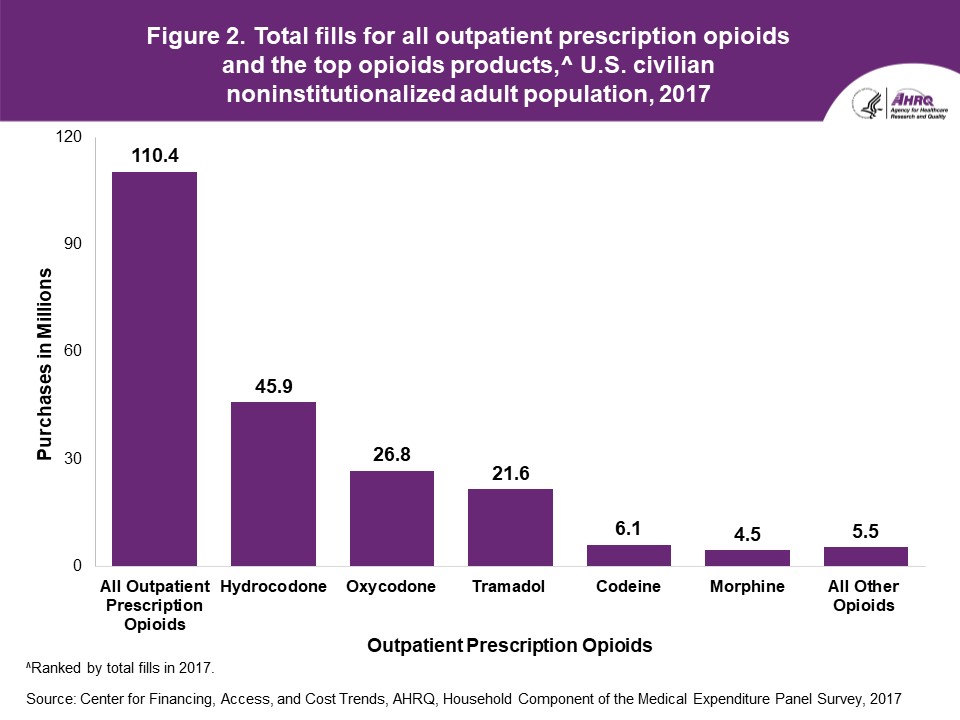
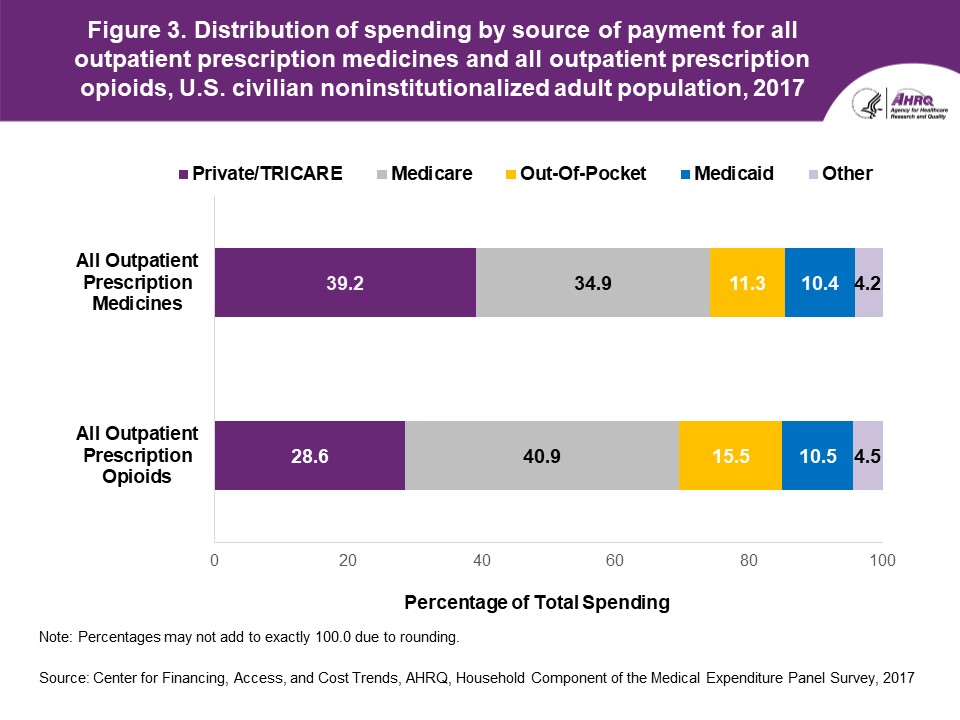
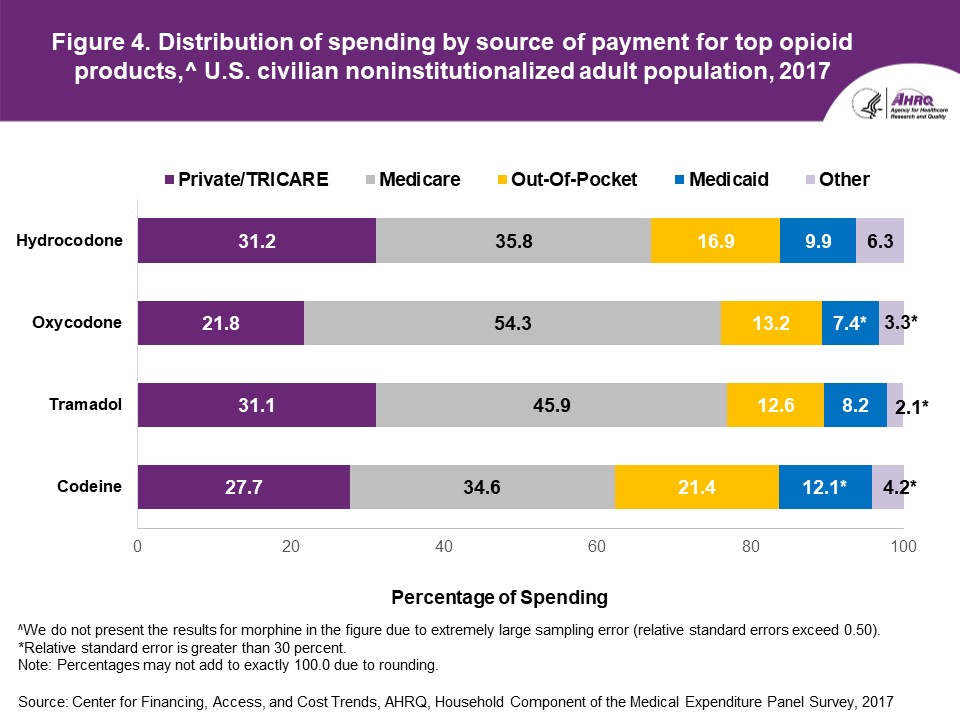
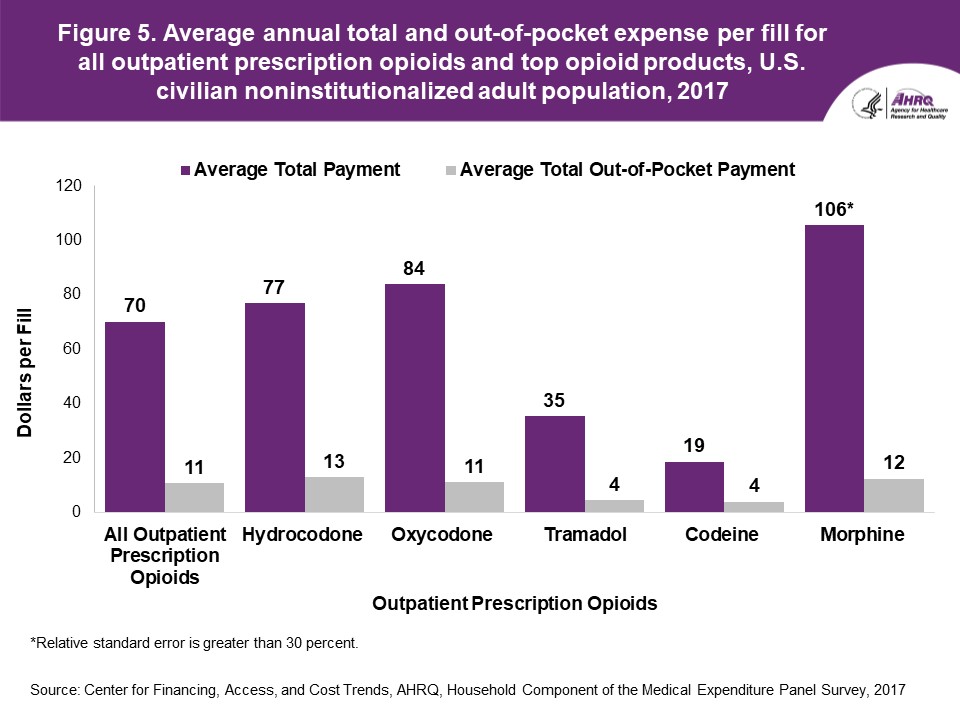
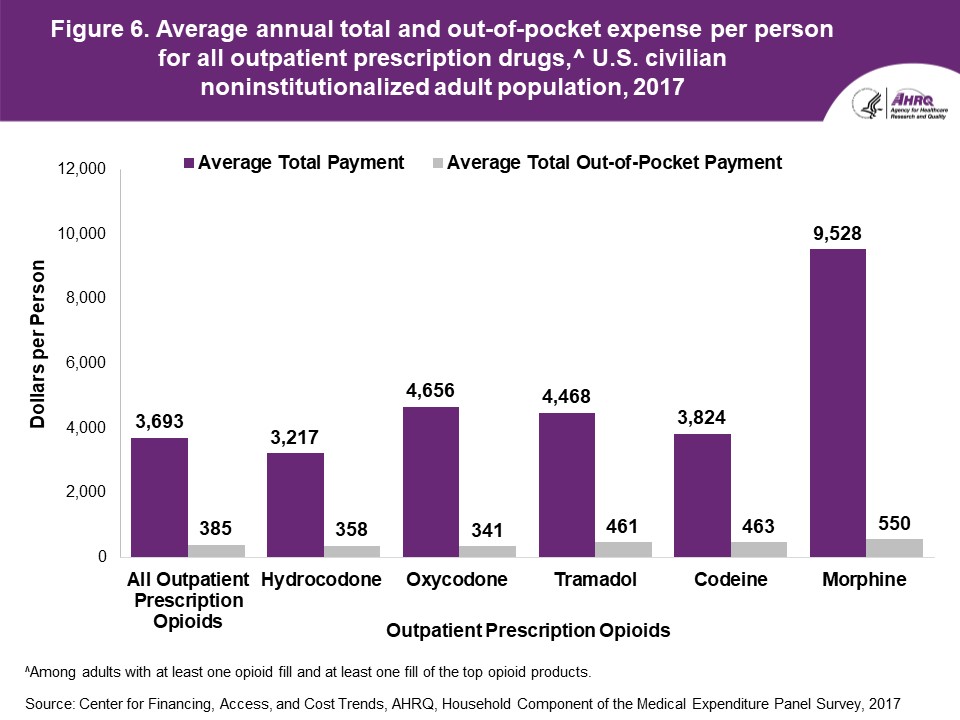
FindingsIn 2017, there was an estimated total of $7.7 billion paid for outpatient prescription opioids purchased by adults in the U.S. civilian noninstitutionalized population (figure 1); 28.8 million adults or 11.5 percent of the 251.1 million adults in the U.S civilian noninstitutionalized population purchased one or more outpatient prescription opioids in 2017 (data not shown). The top five opioid products (active ingredients) ranked by total expenses were the following: Hydrocodone ($3.5 billion), oxycodone ($2.2 billion), tramadol ($0.8 billion), morphine ($0.5 billion), and codeine ($0.1 billion).During 2017, there was an estimated total of 110.4 million opioid outpatient prescription fills which comprised 3.8 percent of all of the 2.9 billion prescription medicine fills (data not shown) for adults in the U.S. civilian noninstitutionalized population (figure 2). The top five products ranked by total fills in 2017 were the following: Hydrocodone (45.9 million prescriptions), oxycodone (26.8 million prescriptions), tramadol (21.6 million prescriptions), codeine (6.1 million prescriptions), and morphine (4.5 million prescriptions). Total outpatient prescription opioid expenses for adults in 2017 were primarily financed by third-party payers: Medicare paid 40.9 percent of total expenses for outpatient prescription opioids, private insurance (including TRICARE) paid 28.6 percent, individuals and family members paid 15.5 percent, Medicaid paid 10.5 percent and other third-party sources paid 4.5 percent (figure 3). For all outpatient prescription medicines, private insurance/TRICARE paid 39.2 percent of total medicine expenses, Medicare paid 34.9 percent, individuals and family members paid 11.3 percent (out-of-pocket), Medicaid paid 10.4 percent, and other third-party sources paid 4.2 percent among adults in 2017. Comparing the distribution of spending by source of payment for all outpatient prescription medicines with spending for opioids (figure 3), out-of-pocket spending comprised a higher proportion of total spending for opioids than for all prescription medicines (15.5 versus 11.3 percent, respectively), while private insurance/TRICARE financed a lower proportion of total spending for opioids than for all prescription medicines (28.6 versus 39.2 percent, respectively). Comparing the distribution of spending by source of payment across four opioid products (hydrocodone, oxycodone, tramadol, and codeine),2 Medicare paid for the highest portion (ranging from 34.6 to 54.3 percent) and private insurance/TRICARE accounted for the second highest portion (ranging from 21.8 to 31.2 percent) of spending for all four products among adults in 2017 (figure 4). Medicaid accounted for the lowest portion (7.4 to 12.1 percent) of spending for the four opioid products. Codeine had the highest proportion of individual and family out-of-pocket payments (21.4 percent), which was significantly higher than that for tramadol (12.6 percent). In 2017, the average annual total and out-of-pocket expenses per fill for all outpatient prescription opioids purchased by adults were $70 and $11, respectively (figure 5). Examining the top five opioid products, morphine had the highest average total expense per fill ($106) followed by oxycodone ($84), hydrocodone ($77), tramadol ($35), and codeine ($19). Hydrocodone, morphine, and oxycodone had significantly higher average out-of-pocket expenses per fill ($13, $12, and $11, respectively) than tramadol ($4) and codeine ($4). During 2017, the average annual total and out-of-pocket expenses per person for all outpatient prescriptions among adults who had at least one prescription opioid fill were $3,693 and $385, respectively (figure 6). Among adults with one or more fills of the top five opioid products, those with any fills of morphine had the highest average total expenses for all outpatient prescriptions per person ($9,528). Those adults with any fills of oxycodone ($4,656) or tramadol ($4,468) had significantly higher average total expenses for all outpatient prescriptions than those with any fills of hydrocodone ($3,217). The average out-of-pocket expenses for all outpatient prescriptions were $550, $463, $461, $341 and $358 per person among those adults with at least one fill of morphine, codeine, tramadol, oxycodone and hydrocodone, respectively. |
||||||||||||||||||||||||||||||
Data SourceThe estimates in this Statistical Brief are based upon data from the 2017 MEPS Full Year Population Consolidated Data File (HC-201) and a non-public version of the 2017 Prescribed Medicines Data File (MEPS HC-197A). |
||||||||||||||||||||||||||||||
DefinitionsExpenses and utilizationUtilization was defined as purchasing (or obtaining) outpatient prescription opioid fills in the year of interest (i.e., 2017 in this Statistical Brief). Refills, as well as original prescriptions, are included in expense and utilization estimates. Expenses include the total direct payments from all sources to pharmacies for prescriptions reported by respondents in the MEPS-HC. Manufacturer rebates to payers and pharmacy benefit companies were not measured and were not subtracted from total direct payments. MEPS estimates of opioid use may differ from estimates based on other data sources for several reasons. For example, MEPS and the Substance Abuse and Mental Health Services Administration's (SAMSHA) National Survey on Drug Use and Health (NSDUH) have substantial differences in methodologies and objectives. The NSDUH estimates for any opioid use comprise both prescribed use and misuse. Misuse includes taking medications for the feeling and in a way that the doctor did not prescribe. NSDUH respondents report use in inpatient settings, as well as outpatient. Moreover, NSDUH includes targeted questions with show cards for specific drugs, is self-reported using audio computer assisted self-interviewing (ACASI), surveys persons aged 12 and older, and questions are asked based on a 12 month recall period. In contrast, MEPS includes only prescribed medicines purchased in outpatient settings (that is, retail and mail-order medicines). Prescription medicines administered in an inpatient setting or a clinic or physician's office are excluded. MEPS data are household reported and one respondent reports for the entire household. MEPS uses computer assisted personal interviewing (CAPI), and questions are asked using a recall period of 3-6 months. Finally, this Statistical Brief reports estimates for adults aged 18 years and older. All opioids and opioid products: Codeine, hydrocodone, oxycodone, morphine, and tramadol Opioids that are commonly used to treat pain are defined using generic drug names for narcotic analgesics and narcotic analgesic combinations in the Multum Lexicon database from Cerner Multum, Inc. We identified slightly more opioids commonly used for pain than one would find in the MEPS public use files due to methods used to preserve the confidentiality of sample members. We excluded opioids not used for pain management from this analysis. These exclusions, which encompass respiratory agents, antitussives, and medicines commonly used in Medication Assisted Treatment, comprise about 8.5 percent of opioid fills reported in MEPS. Age Age was defined using the last available age in 2017 for each sampled person. Adults were defined as persons equal to or greater than 18 years of age. Sources of payment
|
||||||||||||||||||||||||||||||
About MEPSThe Medical Expenditure Panel Survey Household Component (MEPS-HC) collects nationally representative data on health care use, expenditures, sources of payment, and insurance coverage for the U.S. civilian noninstitutionalized population. The MEPS-HC is cosponsored by the Agency for Healthcare Research and Quality (AHRQ) and the National Center for Health Statistics (NCHS). More information about the MEPS-HC can be found on the MEPS Web site at http://www.meps.ahrq.gov/. |
||||||||||||||||||||||||||||||
ReferencesFor a detailed description of the MEPS-HC survey design, sample design, and methods used to minimize sources of nonsampling error, see the following publications:Cohen, J. Design and Methods of the Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 1. AHCPR Pub. No. 97-0026. Rockville, MD: Agency for Healthcare Policy and Research, 1997. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr1/mr1.pdf Cohen, S. Sample Design of the 1996 Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 2. AHCPR Pub. No. 97-0027. Rockville, MD: Agency for Health Care Policy and Research, 1997. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr2/mr2.pdf Cohen, S. Design Strategies and Innovations in the Medical Expenditure Panel Survey. Medical Care, July 2003: 41(7) Supplement: III-5—III-12. Ezzati-Rice, T.M., Rohde, F., Greenblatt, J. Sample Design of the Medical Expenditure Panel Survey Household Component, 1998–2007. Methodology Report No. 22. March 2008. Agency for Healthcare Research and Quality, Rockville, MD. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr22/mr22.pdf Stagnitti, Marie N., Beauregard, K., and Solis, A. Design, Methods, and Field Results of the Medical Expenditure Panel Survey Medical Provider Component (MEPS MPC)—2006 Calendar Year Data, Methodology Report No. 23. November 2008. Agency for Healthcare Research and Quality, Rockville, MD. http://www.meps.ahrq.gov/mepsweb/data_files/publications/mr23/mr23.pdf Sing, M., Banthin, J., Selden, T., et al.: Reconciling Medical Expenditure Estimates from the MEPS and NHEA, 2002. Health Care Financing Review 28(1):25–40, Fall 2006. Internet Address: https://www.cms.gov/HealthCareFinancingReview/downloads/06Fallpg25.pdf |
||||||||||||||||||||||||||||||
Suggested CitationDing, Y. and Miller G.E. Total Expenses, Total Utilization, and Sources of Payment for Outpatient Prescription Opioids in the U.S. Adult Civilian Noninstitutionalized Population, 2017. Statistical Brief #529. April 2020. Agency for Healthcare Research and Quality, Rockville, MD. https://meps.ahrq.gov/data_files/publications/st529/stat529.pdfAHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of health care in the United States. We also invite you to tell us how you are using this Statistical Brief and other MEPS data and tools and to share suggestions on how MEPS products might be enhanced to further meet your needs. Please email us at MEPSProjectDirector@ahrq.hhs.gov or send a letter to the address below: Joel Cohen, PhD, Director Center for Financing, Access, and Cost Trends Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 |
||||||||||||||||||||||||||||||
|
1Bernard, D., Machlin, S.R., Fang, Z., and Cohen, J. Average Annual Opioid Use among Adults Treated for Conditions Associated with Chronic Pain versus Other Conditions, 2013−2015. Research Findings #43. August 2019. Agency for Healthcare Research and Quality, Rockville, MD. https://meps.ahrq.gov/data_files/publications/rf43/rf43.pdf 2We do not report results for morphine in figure 4 due to relative standard errors that exceed 0.50. |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
^Ranked by total expenses in 2017. |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
^Ranked by total fills in 2017 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
Note: Percentages may not add to exactly 100.0 due to rounding. |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
^We do not present the results for morphine in the figure due to extremely large sampling error (relative standard errors exceed 0.50). |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
*Relative standard error is greater than 30 percent. |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
^Among adults with at least one opioid fill and at least one fill of the top opioid products. |
| |||||||||||||||||||||||||||||